



Key Takeaways
- Fragmented healthcare systems limit automation impact. Bots can move data between systems, but they rarely solve the more profound integration problems across EHRs, payer portals, and operational platforms.
- Automation often removed simple tasks but left complex work behind. Human teams still manage exceptions, approvals, and interpretation-heavy processes like prior authorization and clinical coding.
- Rule-based automation lacks decision-making capability. Many healthcare workflows require judgment, contextual understanding, and clinical interpretation that traditional automation cannot handle.
- Automating flawed processes only accelerates inefficiency. Without redesigning workflows, automation can speed up the movement of information while leaving operational bottlenecks untouched.
- The next phase of healthcare automation focuses on decision intelligence. Systems are evolving to analyze data, support operational reasoning, and guide actions rather than simply executing predefined tasks.
Healthcare has spent the better part of the last decade trying to automate itself. Hospitals’ automated scheduling. Revenue cycle teams deployed bots to process claims. Payers implemented automation to verify eligibility and process documentation. If you attended healthcare IT conferences between 2016 and 2023, automation was everywhere in the conversation.
And yet… the results have been oddly underwhelming.
Yes, some administrative costs went down. Yes, staff stopped performing certain repetitive tasks. But the large-scale transformation many executives expected never quite arrived. Operational teams still complain about delays, manual work, and fragmented workflows. The promised efficiency gains often plateau after the first round of automation projects.
When healthcare leaders say automation “didn’t deliver ROI”, they’re rarely talking about technology failures. The bots worked. The integrations ran. Data moved where it was supposed to go.
The problem lies elsewhere.
Most healthcare automation initiatives were built on top of operational environments that were already deeply fragmented, heavily dependent on human interpretation, and almost entirely lacking automated decision-making. In other words, organizations automated activities without fixing the structural conditions that made those activities inefficient in the first place.
Three issues come up again and again when you look closely at automation programs that stalled:
- System fragmentation that automation never really solved
- Persistent human dependency inside supposedly automated workflows
- Almost no real decision-making capability within the automation layer
None of these problems are new. What’s interesting is how consistently they show up across hospitals, payer organizations, and health networks.
Fragmentation: The Automation Layer Nobody Asked For
Walk into any large hospital IT environment and you’ll see a technology ecosystem that grew gradually over decades.
There’s the electronic health record system. Then there are the radiology systems, pharmacy platforms, billing systems, patient engagement tools, insurance verification portals, referral management platforms, and a long list of specialized clinical applications.
Each one solves a particular operational problem. Very few were designed to work seamlessly with the others.
Automation arrived as a way to bridge those gaps. At least that was the expectation. In reality, automation tools often became just another layer sitting between already disconnected systems. Bots log into portals, copy data between platforms, and trigger downstream actions. The work gets done, technically speaking. But the underlying architecture remains just as fragmented as before.
Take insurance eligibility verification, a routine step before almost every patient visit.
It sounds simple when described in a process diagram:
- Retrieve patient information
- Check insurance coverage
- Confirm eligibility
In practice, the workflow is anything but straightforward. Different insurers maintain separate portals. Coverage responses vary widely depending on the policy. Some responses are immediate; others arrive hours later. Occasionally the system simply times out.
Automation bots can collect data from these portals, but they don’t eliminate the fragmentation itself. Staff still need to reconcile conflicting information, chase down missing responses, or validate coverage details manually.
So the automation layer ends up acting like a digital courier moving data around — useful, certainly, but far from transformative.
Human Dependency: The Exception Problem
Automation works best when processes behave predictably. Healthcare workflows rarely do. A large portion of healthcare administration involves interpretation, judgment, and dealing with exceptions. That reality doesn’t disappear just because bots handle the first few steps of a workflow. Prior authorization offers a prime example.
Anyone who has worked in healthcare operations knows how complicated this process can become. Physicians submit clinical information, insurers evaluate medical necessity, and documentation requirements vary widely depending on the treatment and payer.
Automation tools can help gather documentation and submit requests, but the process often runs into situations that it cannot resolve automatically. Maybe the clinical documentation is incomplete. Maybe the insurer requests additional evidence. Sometimes the payer’s requirements changed, and nobody noticed yet.
At that point, humans step back into the workflow. Nurses, care coordinators, and administrative staff review cases, interpret medical notes, and determine how to respond. Automation essentially hands the difficult parts back to people. This creates an odd operational dynamic. The automated system handles routine cases efficiently while humans deal almost exclusively with the complex ones. That might sound reasonable — until the volume of exceptions grows.
And in healthcare, exceptions tend to grow quickly. Some hospitals discovered that once automation accelerated intake processes, the number of exception cases actually increased. Staff suddenly found themselves handling larger queues of complicated cases without the simple tasks that once balanced their workload.
Automation removed the easy work but left behind the hard decisions. It’s not exactly the efficiency gain organizations expected.
The Missing Ingredient: Decision Capability
If you look closely at many healthcare automation platforms, a pattern becomes obvious. They follow instructions extremely well. They rarely make decisions. Traditional automation systems rely on predefined rules. If a particular field contains a certain value, the system triggers a specific action. The workflow continues if the data matches a known format. Otherwise, the process stops.
Healthcare rarely fits into neat rule sets. Consider medical coding, a task that converts physician documentation into standardized billing codes. Automation systems can extract structured data from documents, but understanding clinical language is a different challenge. A physician might describe symptoms, possible diagnoses, or uncertain findings. Coders interpret these notes within the context of clinical guidelines and billing regulations.
A rule-based system struggles in those situations. It either makes incorrect assumptions or escalates the case for manual review.
And so the workflow slows down again.
You see similar limitations across multiple administrative processes:
- Claims denial management
- Care coordination prioritization
- Referral triage
- Documentation validation
Automation retrieves data. Humans determine what it means. Which raises an obvious question: if humans still make the critical decisions, can the workflow truly be considered automated?
For years, healthcare organizations focused on automating tasks rather than enabling automated reasoning.
That approach inevitably reached its limits.
When Automation Speeds Up the Wrong Process
In many organizations, automation initiatives begin with the goal of improving efficiency and reducing manual effort. However, when we apply automation to processes that are already inefficient or overly complex, we simply accelerate the existing workflow instead of improving it. As a result, organizations sometimes end up moving the same flawed process faster rather than transforming it.
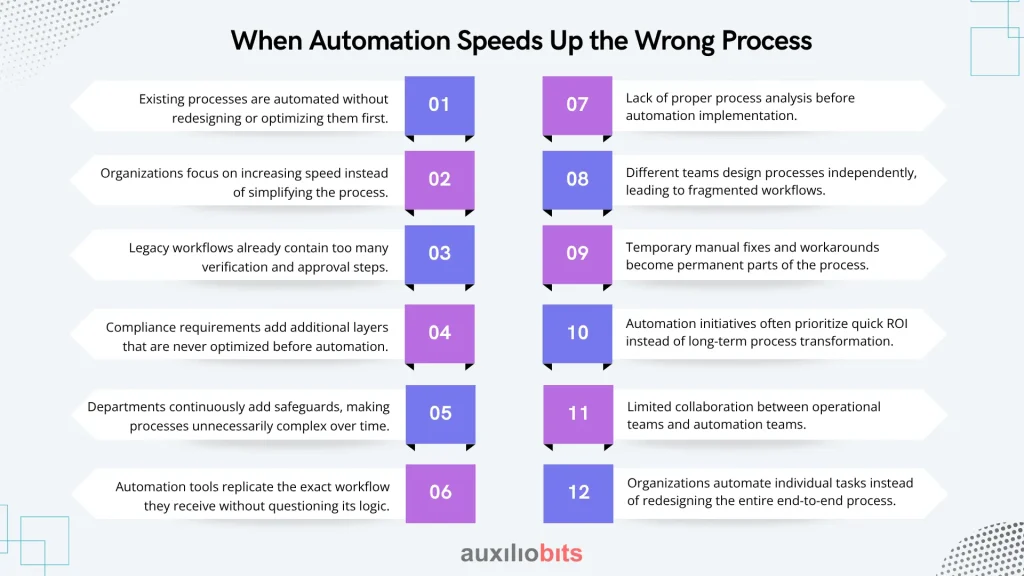
Key Reasons:
- Existing processes are automated without redesigning or optimizing them first.
- Organizations focus on increasing speed instead of simplifying the process.
- Legacy workflows already contain too many verification and approval steps.
- Compliance requirements add additional layers that are never optimized before automation.
- Departments continuously add safeguards, making processes unnecessarily complex over time.
- Automation tools replicate the exact workflow they receive without questioning its logic.
- Lack of proper process analysis before automation implementation.
- Different teams design processes independently, leading to fragmented workflows.
- Temporary manual fixes and workarounds become permanent parts of the process.
- Automation initiatives often prioritize quick ROI instead of long-term process transformation.
- Limited collaboration between operational teams and automation teams.
- Organizations automate individual tasks instead of redesigning the entire end-to-end process.
What Is Starting to Change
should actually work. There’s growing recognition that replicating human actions — clicking through portals, copying data fields, and submitting forms — only addresses a small part of the operational problem.
The more meaningful opportunity lies in automating decision support within workflows. Instead of simply collecting eligibility data, systems can analyze coverage rules and determine whether verification is necessary before initiating the process. Rather than flagging claims denials for manual review, systems can analyze denial patterns and recommend corrective actions automatically. This shift moves automation from task execution toward operational reasoning. It’s not perfect yet, but the direction is clearly different from the first generation of healthcare automation tools.
Rethinking the Role of Automation
The organizations that are beginning to see stronger returns from automation tend to approach it differently.
They start by examining the process itself.
Questions that often emerge during these reviews include:
- Where are the real decision points in this workflow?
- Which steps exist purely because systems don’t communicate well?
- What information is actually required to move the process forward?
- Where do experienced staff apply judgment today?
Once those questions are answered, automation can be designed around decision points rather than mechanical steps.
For example, referral automation can include clinical prioritization logic. Claims automation can analyze patterns in historical denials. Care coordination workflows can automatically identify high-risk patients based on multiple data sources.
Automation becomes less about performing tasks and more about guiding operational decisions. That distinction changes the economics of automation programs quite significantly.
Automation Isn’t Replacing Humans — It’s Changing Their Role
There’s another subtle shift happening within healthcare organisations that are adopting more advanced automation approaches.
Human involvement doesn’t disappear. It changes. Instead of assembling information manually, staff review system recommendations. They evaluate cases flagged as high-risk or complex rather than chasing missing documentation.
In other words, the automation layer performs the investigative work that previously consumed large portions of administrative time. Humans remain responsible for oversight and complex judgment — which, frankly, is where their expertise is most valuable anyway. This hybrid model tends to work better in healthcare environments where uncertainty and variation are unavoidable.
Also read: Healthcare Authorization Automation Using OpenAI + UiPath
The Real Lesson Healthcare Learned
Looking back, the early years of healthcare automation were somewhat optimistic about what rule-based systems could accomplish.
Organizations believed that repetitive administrative work was the main source of inefficiency. But the more profound problem was always structural complexity. Fragmented systems. Inconsistent data. Processes built around human interpretation rather than standardized decision logic.
Automation addressed the visible symptoms — the manual steps — but did not resolve the deeper causes. Now the industry seems to be adjusting its expectations.
Automation is no longer viewed simply as a way to eliminate repetitive tasks. Increasingly, it’s considered a way to support operational reasoning across fragmented systems and unpredictable workflows.
That shift may finally allow healthcare automation to deliver the kind of ROI organizations expected all along. It just took the industry a while to realize that moving data around was never the real challenge.





